What does the field of ‘international disaster management’ have to teach us about the United Kingdom’s response to the CoVid-19 pandemic?
The United Kingdom is currently experiencing the highest per capita mortality rate in the world from the CoVid-19 coronavirus. This could yet be reduced if some of the key lessons coming out of the field of ‘international disaster risk management’ were applied, including from the Ebola responses in Sierra Leone and the Democratic Republic of Congo between 2014 and 2018. In summary, the main ones are:
- Treat pandemics as full-on ‘natural’ disasters and reconfigure the decision-making architecture accordingly
- Evaluate performance regularly and transparently
- Engage the public via a credible spokesperson, leaving Ministers to explain political decisions
- Be consistent and coherent with risk communications
- Enhance tertiary and social care capacity
- Enhance diagnostic capacity, especially rapid diagnostic testing
- Localise the response through bottom-up engagement with communities and local authorities
- Incentivise self-isolation through financial compensation and job guarantees
- Provide cash transfers, not food
- Vaccine ‘wars’ over price and priority are inevitable. Manage expectations over vaccine development, efficacity and distribution
- Don’t rely on untested technology, especially mobile phone apps
- Ensure the mass media understands its social responsibility during a national emergency and re-roles accordingly. Establish a dedicated 24/7 YouTube channel (see Points 3 and 4)
Pandemics (or major cross-border epidemics) should be conceived of as ‘natural’ disasters rather than outbreaks of disease from the outset. This will ensure the change of mindset required by politicians, the public, and the health community to acknowledge that coordination should encompass multiple sectors and technical disciplines beyond those related solely to medicine and public health. Disasters are not inevitable; they are the result of decades of accumulated risk and deliberate decisions taken or not taken by society as a whole. In this, disasters are social constructs. In recognition of these factors, a reconfiguration of the decision-making architecture beyond everyday crisis management is required so that scientific evidence not only influences political decision-making but is seen to do so. Full engagement of all the sectors and disciplines involved will need the strategic oversight of an independent disaster risk management adviser. At no time was such a person involved in the UK response.
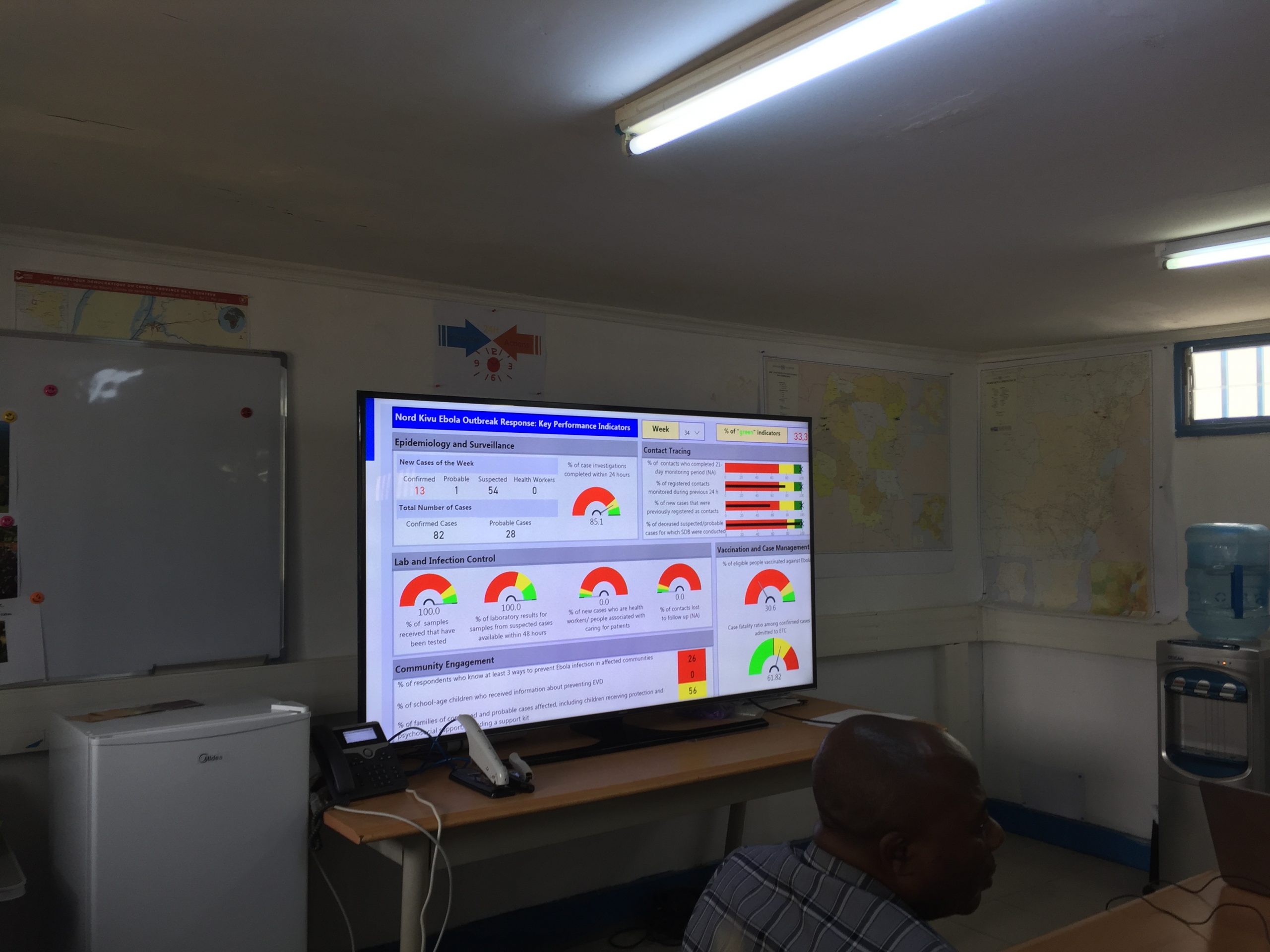
Hold regular real-time evaluations and periodically review performance. UN guidelines exist for this. In fact, in any major disaster response the British government would be the first to complain if the UN did not apply these guidelines. Measure performance against the counterfactual – the model of predicted outcomes that would probably occur if nothing were done – and use ‘net excess mortality all-cause’ and QALYs to justify the opportunity costs involved in health outcomes, not just mortality rates. Publish the dashboard so that everyone can see things like laboratory tests conducted, bed occupancy rates, vaccine deployment, therapeutic development, and ambulance usage in one place. To the extent possible, allow access to the underlying meta-data.
A credible spokesperson fosters trust in a way that a politician cannot. This would not normally be a chief medical officer as the response is not only medical. Nor would it normally be a chief scientific adviser as much of the evidence is anecdotal rather than ‘scientific’. The public need to know the limitations of ‘the science’ and ‘the science’ needs to inform – not lead – political decision-making. Attaching high, medium and low indicators of confidence to ‘facts’ which are actually opinions would help build public trust. Scientists rarely agree completely. David Nabarro of WHO, Jeremey Farrar of the Welcome Foundation or Mukesh Kapilla of Manchester University, all of whom have real-world experience not just of outbreaks, but of disaster management, academia and science, would have the kind of profile needed.
Risk communications is not the same as ‘Strat-Comms’ (strategic communications) and needs to be STARCC (strategic, timely, actionable, relevant, consistent, and coherent). Messaging is more effective when coming from trusted sources, including celebrities. It’s about addressing rumours and the inconsistencies of human behaviour, not just the implacable rationality of epidemiological data. Every word matters. ‘Boosterish’ dissembling by politicians undermines public health messaging. The public were very quick to spot that vaccines “offered” mean something very different to vaccines “given,” for example. Technical issues like the sensitivity & specificity of rapid diagnostic tests should be explained in detail. It is only this level of knowledge that leads the public to understand how vaccination coverage, however high it is and however effective the vaccine, means that those vaccinated “do not become invincible overnight.” Don’t blame the public if messages like this have not been understood. Consider changing the school curriculum.
Signal that decision-makers understand the difference between the Hippocratic imperative of saving every individual life versus the public health imperative of saving populations. Wearing or not wearing of face-masks is more about this difference than it is about the type of mask or the opportunistic risk of putting them on and taking them off.
Over-centralisation should be avoided, especially as it means introducing inexperienced private-sector partnerships. This means that contact tracing and laboratory diagnostics should be conducted as close to affected communities as possible, preferably by government-led public health services whose capacities have been enhanced.
Pharmaceutical companies are not charities. They are in competition and will only invest in public goods if incentivised to do so, including guarantees that R&D costs will be underwritten by government in exchange for ‘no-profit’ distribution for a limited period. Because of this investment of public money, terms of commercial contracts should be in the public domain. They should not be expected to develop vaccines on a not-for-profit basis, although they should be expected to support equitable distribution. Overt and covert manipulation of research data should be expected. Usually, vaccine efficacity data from clinical trials is not emulated in the real-world and there can be considerable lags in production, which means that public and political expectations over when and how much immunity is conferred through mass immunization need to be managed.
Be wary of un-tested technology, especially when it involves mobile phone apps which, like cash transfers, are fragile at the best of times. Mobile phones, however, have a major role to play in coherent risk communications, especially when linked to location. The Red Cross are world leaders in this.
The media – all of it, not just public broadcast media – has a social responsibility during a pandemic response and needs to re-role accordingly. Absolute and Relative figures should always be used to avoid giving a false impression of what is going on. When the ‘science’ is open to interpretation, expectations need to be managed accordingly. TV and Radio hosts and their producers should take extra care to avoid creating false narratives through provocative framing of apparently innocent and binary questions and then holding politicians to account for “over-promising and under-delivering”. This is not accountability, this is sensationalism. And it can quickly confuse the public and erode trust in the wider effort. All so-called ‘facts’ promulgated via social and mass media should come with a ‘confidence indicator’ attached (as the IPCC does when reporting on climate change, for example). Consideration should be given to establishing a dedicated TV and Radio channel
End
James Shepherd-Barron is a practising international disaster risk management consultant who advised the British government on its Ebola responses in West Africa during the period 2014-2018. He is a Professor of International Disaster Management at Fordham University in New York and author of Absolute Disaster.